Pectus excavatum put pressure on her ability to breathe
Thanks to surgery, the only pressure Kinley feels now is the need to play her best. Watch her story below.

Pectus Excavatum and Pectus Carinatum
One of the biggest questions we get asked is what is the difference between pectus excavatum and pectus carinatum? While there is a difference, it's important to know that they are both chest wall deformities.
A chest wall deformity is an abnormal development in the chest wall. The condition is fairly common and the abnormality can vary from mild to severe. These deformities are more common in boys and in Caucasians. Up to 40 percent of patients will have an affected family member and several monogenic syndromes are associated with pectus deformities including Marfan syndrome, homocystinuria and Ehlers-Danlos syndrome. It can either be present at birth or not develop until puberty.
The two most common congenital chest wall deformities fall into the categories of pectus carinatum (sometimes called pigeon chest or sternal protrusion) and pectus excavatum (also called funnel chest or sunken sternum). Depending on the type of pectus and diagnosis, treatment may be surgical or nonsurgical, depending on the level of severity. For children with pectus excavatum, chest wall deformities may range from mild to severe. Mild cases might be barely noticeable. Pectus excavatum can be completely harmless, but the visual appearance can affect a child's self-image, and they may also be subjected to teasing and even bullying. Severe cases can cause a deep hollow in the chest and may affect the heart and lungs. Surgery can often correct the condition and treat any heart or lung issues. In pectus carinatum, the chest wall can protrude, or stick out. It can sometimes cause chest pain. For most patients a compression brace can correct the protrusion. In some cases surgery may be needed.
We're here to help.
If your child requires surgery, you probably have lots of questions. We can help.
If you would like to speak to our staff, please call our offices today!
Jack's story - Pectus excavatum
"It's almost like you changed out a LEGO piece. Like you put in a different middle body but kept the same legs and head. It felt strange, but instantly it felt like I had space to breathe."
— Jack (17 years old)

Kinley's story
"I wanted to share our success story with you and Dr. Iglesias. Our daughter, Kinley, had surgery in July 2020 and even though her recovery was a long and tough one, I'm happy to share that she was able to come back and compete at the Texas Class 4A State Cross Country meet in November and is now a back-to-back state champion! Truly our favorite "gold" medalist and thankful to your team at Cook Children's for giving her this opportunity."
— Kimberly (mother of Kinley)
Ben's story - Pectus carinatum
"This has been a big growing experience for Ben. In his easy life, he hasn’t had many challenges to overcome, and I’ve loved watching him learn confidence and empathy through this one. We appreciate the way Dr. Knott handled everything with Ben - so honest and straightforward yet caring. Thank you."
— Shannon (Ben's mother)

For children with pectus excavatum, chest wall deformities may range from mild to severe. Mild cases might be barely noticeable. Pectus excavatum can be completely harmless, but the visual appearance can affect a child's self-image, and they may also be subjected to teasing and even bullying. Severe cases can cause a deep hollow in the chest and may affect the heart and lungs. Surgery can often correct the condition and treat any heart or lung issues.
Who gets it?
Pectus excavatum affects about 1 in 400 children, and is most common in males although females can be affected as well. Up to 40 percent of patients will have a family member, typically a parent or grandparent, who also has it, but there is no clear genetic link. There are several monogenic syndromes associated with pectus deformities including Marfan Syndrome, Homocystinuria and Ehlers-Danlos Syndrome. It can either be present at birth or not develop until puberty.
 |
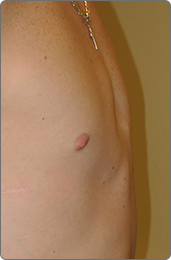 |
Male, before and after

Female, before and after
What causes it?
It is generally regarded as a genetic condition, based on the fact that it is usually present in several members of the same family and is often associated with other genetic diseases; however, its causes remain in debate.
What are the symptoms?
Common symptoms of chest wall deformities are:
- Sunken appearance in the chest.
- Shortness of breath.
- Decreased stamina during exercise.
In addition, your child may also have chest pain related to abnormal bone and cartilage growth. Pectus excavatum typically gets worse with age or during growth spurts that occur during adolescence.
How is it diagnosed?
Workup of pectus excavatum includes your child's medical history and a physical exam, along with one or more of the following tests:
- Chest X-ray.
- CT scan of chest.
- Cardiac ECHO.
- Pulmonary function test (PFT).
- Testing for possible nickel allergy.
- Cardiac MRI.
How is it treated?
Treatment of mild pectus excavatum may consist of exercises for improving posture and upper body strength. If your child has moderate to severe pectus excavatum, surgery may be recommended.
Nonsurgical options
For mild deformities, posture control, exercise program (e.g., deep breathing, pushups) and annual follow-up may be appropriate. Many patients are candidates for this non-operative treatment before considering surgical repair. Compliance is important for optimal results.
Surgical options
The timing of surgery is dependent on your child's age, symptoms and anatomy. Surgical options are generally deferred until mid to late adolescence–if symptoms allow–to prevent problems with chest wall compliance which may occur if done in younger patients.
Pain control and comfort
Multimodal pain control with the anesthesia pain team, and also offering intra-operative Cryo Nerve Block for 1-3 + months of post-surgical relief allowing a more rapid recovery and shorter hospitalization.
Cryo Nerve Block technology uses a unique freezing method to temporarily block pain signals from nerves in the affected area, providing an effect that’s similar to a local anesthetic.
Nuss minimally invasive repair of pectus excavatum (MIRPE)

- Uses small lateral chest incisions and a thoracoscope to place a curved stainless steel bar underneath the ribs and the sternum.
- No excision of cartilage is needed.
- The bar is removed in two to three years as an outpatient procedure.
- Most patients are candidates for this procedure, but some very asymmetric deformities may require other approaches.

Ravitch repair*
- A longer anterior thoracic incision is used to excise the abnormally shaped cartilages in a subperichondrial plane.
- An osteotomy is often made in the sternum to position it appropriately.
- A stainless-steel bar is placed to keep the sternum in position while the cartilage grows to the sternum (approximately two years).
- Some patients may be candidates for more limited resections.
Who gets it?
Pectus carinatum is less common than pectus excavatum. Only a fifth as many children have it. It is more common in in boys – only 1 in every 4 patients diagnosed with this condition are girls. It generally appears later than excavatum deformity (50 percent by 11 years of age). This condition also worsens during puberty.
What causes it?
It is generally regarded as a genetic condition, based on the fact that it is usually present in several members of the same family and is often associated with other genetic diseases; however, its causes remain in debate.
What are the symptoms?
Common symptoms are:
- Chest wall may protrude forward, thus the name pigeon chest.
- Chest wall may also be asymmetric meaning one side my protrude forward and the other may sink in (like excavatum).
- It is associated with congenital heart disease, but it is less likely to have cardiopulmonary symptoms.
- In addition, your child may also have chest pain.
How is it diagnosed?
Workup includes your child's medical history and physical exam. Less common, one or more of the following tests are performed:
- Chest X-ray.
- CT scan of chest.
- Cardiac ECHO.
How is it treated?
Surgical repair is an option for people with severe pectus carinatum, but a compression brace can be used to help flatten the chest in most patients. The pectus compression brace is a custom brace made by Cook Children's Orthotics and Prosthetics. This is a preferred treatment for children whose bones are still growing. The brace is worn 16-23 hours a day for the first year and 12-16 hours for the second year. Many patients are candidates for this non-operative treatment before considering surgical repair. Results are often seen in just a few months, when worn according to instruction. Correction is faster and more complete for younger children.
Ravitch repair
- A longer anterior thoracic incision is used to remove the abnormally shaped cartilages under the connective tissue (a subperichondrial plane).
- An osteotomy (surgical sectioning of the bone to shorten or lengthen it) is often made in the sternum to position it appropriately.
- A stainless-steel brace is placed to keep the sternum in position while the cartilage grows to the sternum (approximately two years).

Post-operative pectus information
After surgical repair of your pectus deformity, you will have a steel bar that is positioned across the chest under the breast bone. The bar usually stays in for 2-3 years.
Please follow these instructions to minimize changes or problems with the bar:
- Your child will be sent home with oral pain medication.Sometimes a stool softener is recommended as well.
- Only light activities of daily living for the first 4-6 weeks after surgery.
- Daily deep breathing/breath holding exercises recommended.
- No contact sports, gymnastics or golf swings for the first 3 months.
- No bending at the waist (use your hips), twisting or slouching for the first month.
- Good posture for life.
- No heavy lifting (backpacks included) for 2 months.
- Daily walks are encouraged immediately following surgery in order to help the child regain strength.
- Child will need to sleep on his/her back for the first month.
- May submerge incisions at 1 week after surgery, may shower 3 days after surgery.
- Children are typically able to return to school two-three weeks after surgical repair.
Additional information
- If you need Magnetic Resonance Imaging (MRI) in the future, inform the radiologist about the bar. It can usually still be performed.
- CPR can still be performed if needed, however, compressions require more force than normal due to the steel bar.
- Defibrillation for cardiac arrest may be performed if needed with the bar in place but the pads need to be positioned front to back.
- You will be given a card stating you have a steel implant. Medical alert bracelets or other reminders may be obtained at www.medicalert.org or other providers.
When to call the doctor
- Coughing that won't stop.
- Increased pain.
- Fever greater than 100.5 F.
- Respiratory distress (difficulty breathing).
- Any signs of infection from the incision site (redness, swelling, and/or pus like drainage).
Meet our team





We're here to help.
If your child requires surgery, you probably have lots of questions. We can help. If you would like to speak to our staff, please call our offices at 682-885-7080.